
Counselors must be sufficiently competent to offer their services to the client. Web (sample) standard authorization for disclosure of mental health treatment information. The protected health information to be disclosed includes the following: While this template is designed to be filled in by patients, it is useful for all kinds of mental health practitioners as well. For the purpose of (provide a detailed description):
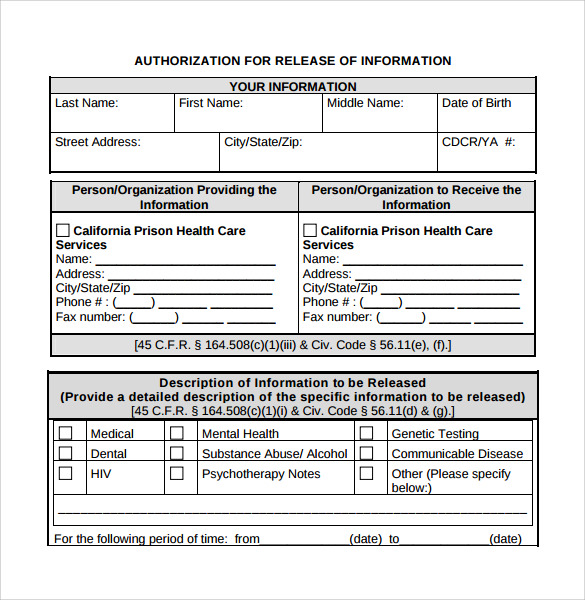
The mental health single point of access provides a single entry point. Authorization for release of information. Web who can use this printable mental health release of information form (pdf)? For hospital records, contact the records manager or patient services manager at the relevant hospital trust.
You can call us for free on 0800 328 4444. Full treatment record including all health/mental health information [2 full treatment record excluding the following information: Ellie mental health 1370 mendota hts rd mendota hts, mn 55120 phone:
Mental Health Release Of Information Form Template

Full treatment record including all health/mental health information [2 full treatment record excluding the following information: Previous treating therapist, current health care providers, parents or school) client name(s): I, _______________________________[insert name of patient/client], whose date.
Free Mental Health Release Of Information Form

Get urgent help now for mental health find an nhs talking therapies service feelings, symptoms and behaviours read about common feelings and symptoms such as stress, anxiety or a low mood. Web i may refuse.
Sample Release Of Information Form Mental Health Classles Democracy
For the purpose of (provide a detailed description): Psychological therapies for people with severe mental health problems (also referred to as severe mental illness) are a key part of the new integrated offer for adults.
30 Medical Release Form Templates ᐅ Templatelab Mental Health Release

Previous treating therapist, current health care providers, parents or school) client name(s): Section vi, please sign (or mark) and date. You can call us for free on 0800 328 4444. The mental health single point.
FREE 17+ General Release of Information Forms in PDF Ms Word

Ellie mental health 1370 mendota hts rd mendota hts, mn 55120 phone: This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private.
Free Release Of Information Form Mental Health Template Doc

Find information and support for your mental health. This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private records need to be.
FREE 9+ Sample Release of Information Forms in MS Word PDF

Mercy medical group behavioral health department, 1792 tribute road, suite 350, sacramento, ca. Web authorization for release/exchange of information. My refusal will not affect my ability to obtain treatment or payment or eligibility for benefits..
Find information and support for your mental health. Type of records to be released and approximate date(s) of service (check all that apply): Free release of information form. This form provides your therapist with written permission to communicate with other individual providers regarding your treatment (e.g. If you need urgent help or are in a crisis, get help or advice from our trained mental health advisors.
Web the purpose of this disclosure of information is to improve assessment and treatment planning, share information relevant to treatment and when appropriate, coordinate treatment services. Release information to obtain information from exchange information with the person/organization in section 3. Section vi, please sign (or mark) and date.
For The Purposes Of C] Treatment/Continuing Care Billing Or Insurance Claims Legal Proceedings Other:
My refusal will not affect my ability to obtain treatment or payment or eligibility for benefits. Web to release, discuss, or disclose the following: ☐coordination of care ☐legal ☐personal ☐other (must specify) _____ information to be disclosed: Web release of information consent form 1.
Web We've Created This Example Consent Form Which You Can Use To Help You Make Sure You Collect The Information You Need.
This template can be used to coordinate the release of confidential information during a client's transition of care or other cicrumstances where private records need to be shared. I, the undersigned, understand that a copy of this signed authorization form is as acceptable as the original. Full treatment record including all health/mental health information [2 full treatment record excluding the following information: Free release of information form.
This Form Can Be Provided To Patients By:
Counselors must be sufficiently competent to offer their services to the client. You should tailor it according to the context and needs of your organisation. For example, your gp practice, optician or dentist. Web release of information form.
Web Authorization For Release/Exchange Of Information.
If the purpose is other than marketing, sale of information, research or as specified above, please specify: Section vi, please sign (or mark) and date. Release information to obtain information from exchange information with the person/organization in section 3. Web getting copies of medical records.
If the purpose is other than marketing, sale of information, research or as specified above, please specify: I may revoke this authorization at any time, but i must do so in writing and submit it to the following address: Web authorization for the release of information is not sufficient for this purpose for client records applicable under federal law 42 cfr part 2. My refusal will not affect my ability to obtain treatment or payment or eligibility for benefits. Web who can use this printable mental health release of information form (pdf)?